☰
Explorar
Iniciar sesión
Crear una nueva cuenta
Pubblicare
×
Descargar
No category
Document
Male Participants Needed! - Male Caregivers of Breast Cancer
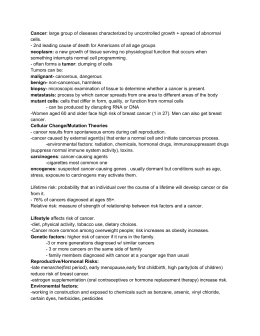
April is Cancer Awareness Month What is Cancer?
Cancer: large group of diseases characterized by
Buenos Aires, 31 de agosto de 2010
Manos de Apoyo Helping Hands Patty Molina, Prevention Manager
Dismantling Racism and a case study: Greensboro CCARES
Bio 242 Unit 4 Lecture 4 PP
Slide 1
SJRA Mammogram Hx Form vSpanish
TAMU–UT Southwestern Partnership for Breast Imaging and
5200 Folleto A5 ISAPS 10
Slide 1
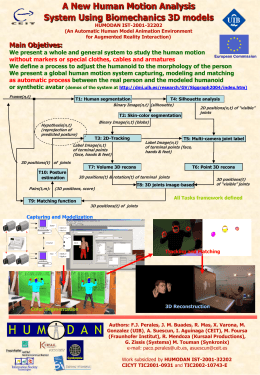
Análisis Estadístico Multivariante de Medidas de la Cara
Mediation between People, Languages, Cultures, and
2007 年 臺灣地區(含金馬)主要死亡原因 死亡原因 死亡 …
Breast Health Patient Navigation Program
Galactorrhea in a 23 year old Male
Gene Ontology - Society of Toxicology
Document
Breast Cancer Survivorship Program Integration with Community
Document
Living With Breast Cancer