☰
Explorar
Iniciar sesión
Crear una nueva cuenta
Pubblicare
×
Descargar
No category
No Slide Title
Ruby on Rails Evaluation – Cognitive Dimensions
High Risk Medications
General Pharmacology - Chemeketa Community College
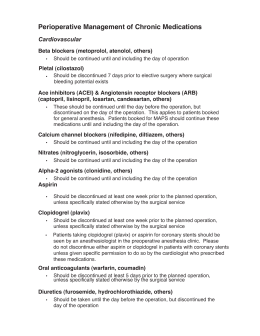
Perioperative Management of Chronic Medications
Assessing and Improving the Transfer of Patient Care
Capítulo doce: Una gira
RUG-ADL & AKPS Assessment - University of Wollongong
Assessing and Improving the Transfer of Patient Care
CS/CIS 130: Introductory Web Programming
Website Design For Your Layout or Club
Practical Pearls to Manage Patients With Swallowing
Developmental Sequence for concepts and skills related to
Slide 1
Psychosocial
Verbos Reflexivos
lumix dmc fz28 manual espaol
All You Wanted to Know About Medications But Were …
Guide rollers
The Two Faces of Depression: Withdrawn or Aggressive
Promoting the Independence of Older Adults
Chap 5 Dosage Forms, Routes of Administration