☰
Explorar
Iniciar sesión
Crear una nueva cuenta
Pubblicare
×
Descargar
No category
Documentation of Nutrition Care
MASTER SYLLABUS
AFHK Presentation
Nutrient Delivery
Missions, Objectives and Logic Models
NUTRITION - University of Lethbridge
Slide 1
Breaking down the barriers: a look at *Por la Salud de Nuestros Ninos*
DETERMINE Your Nutritional Health
Slide 1
Nutrition Therapy and Dialysis
Basic Human Nutrition Lecture 1
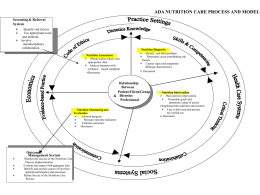
The Nutrition Care Process: Diagnosis, Intervention
Slide 1
Slide 1
Nutritional Support Study Session for HCSW in practice
Nutrition Care Process: Assessment
No Slide Title
Economic tools to evaluate social science programs …
European Commission DG Health and Consumers …
Title of Presentation Name of event
Codex Alimentarius: Costa Rica
Español III